Double Incision Vs. Keyhole
The two most common types of top surgery are:
1) Double Incision mastectomy (most common), and
2) Keyhole mastectomy.
Dr. Mckee performs both of these techniques, as well as other customized techniques. For the double incision technique and keyhole technique, there are different advantages and disadvantages.
We do not use drains for any of our techniques. Instead, we use special internal dissolving stitches (called progressive tension sutures) that secure the underside of the skin to the chest muscle envelope (fascia). Dr. Mckee learned this technique while training in Toronto with Dr. Hugh Mclean. We also require you to wear a surgical compression binder for 1 month after surgery to counteract the swelling under the skin. In this way, we avoid the discomfort of the drains and the scars at the drain site. Drains can also be a source for infection after surgery. We do not require drains for any of the top surgery techniques that we use.


Double Incision Surgery
The Double Incision Technique is most commonly used technique around the world. It is a reliable technique that can be used for all different body shapes and sizes. The two most common subtypes of this technique are 1) double incision mastectomy WITH nipple grafts, and 2) double incision mastectomy WITHOUT nipple grafts.

Before and After photos: 1 Year after tops surgery (double incision mastectomy WITH nipple grafts)
In contrast, this hypothetical patient had a double incision mastectomy WITHOUT Nipple grafts. After everything has settled, they may choose to obtain nipple tattoos, a large chest tattoo design, or leave it blank.
On each side of the chest, an ellipse of tissue is drawn and then removed surgically in one big piece for each side. The removed tissue includes skin, fat, glandular tissue, and the nipples. This is a mastectomy. This creates 2 surgical openings. The underlying muscle is left untouched. The remaining skin on the top is stretched downward, and the remaining skin on the bottom is stretched upward. This creates 2 long horizontal scars. These scars typically starts 3cm from the midline of the chest, and go all the way to the side of the chest.

Illustration describing how the double incision mastectomy works.
Regarding scar appearance, some patients prefer a straight line scar, while other patients prefer a scar that swoops upwards slightly towards the armpit. We are able modify the scar shape based on patient preference (within reason, and within the limits of their skin quality and body shape/size). The surgeon tries to avoid creating a scar that spans across the midline of the chest whenever possible, however rarely it is necessary to prevent a pump of excess skin or fat from forming. Risks for this include a) poor skin quality, and 2) left and right breast tissue being situated very close together along the midline of the chest.
People have different preferences about nipple reconstruction. Some patients choose to have nipple grafts (or nipple skin transplants). In the case of nipple grafts, Dr. McKee will speak with you about your goals for nipple appearance. The nipples are generally made smaller in diameter (and projection) and then transplanted on to the chest in a new position where they weren’t before. The goal is to create a flatter (more natural) appearing nipple that accompanies a flatter chest overall. Nipple grafts are fragile for about 2 weeks after surgery and require a little extra care. Less than 3% of the time, a nipple graft fails (the nipple skin doesn’t survive ). If that happens, the patient ends up with a circular ~2cm wound that heals as a circular scar within a couple weeks.
During the procedure itself, Dr. Mckee choses where the nipple grafts go on the chest. This decision is based on measurements and experience. We are happy to involve you in this part of the decision making. Sometimes however, one side of the chest can shifts (or scar) a little differently after surgery and healing. This means that the nipples may not be in the perfect (desired or symmetric) position. Everyone heals a little differently. This is a rare potential complication of nipple grafts. Choosing between nipple grafts and no nipple grafts is a personal decision, and we can help you decide during the consultation. We are prepared to do whichever option you chose. Remaining nipple sensation is expected to be fairly minimal with either option.

Illustration of how the nipple grafts are created for those patients that choose to have double incision mastectomy WITH nipple grafts
Alternatively, some patients choose not to have nipple grafts at all, and may choose nipple tattoos once their healing is complete. Nipples tattoos on the chest can be performed safely 3-6 months after surgery.

Illustration of how the surgery works for those patients that chose to have double incision mastectomy WITHOUT nipple grafts
After everything has settled(3-6 months), patients that chose the no-nipple-graft route (blank chest) may choose to 1) obtain nipple tattoos, 2) obtain a large chest tattoo piece design (wait 12 months before tattoo on the scar itself though), or 3) leave the chest blank. In our experience, this is particularly a common option for patients that are non-binary, or have had previous breast reduction surgery, or have a very large amount of chest tissue to be removed.

This is an example of a nipple tattoo. With the medical tattoo artist, the patient can describe their goals for the appearance of the nipple and areola regarding: size, shape, color, 3D look, texture, and location on the chest.

This is an example of a patient who had double incision mastectomy WITHOUT nipple grafts, but later had nipple tattoos placed after the swelling and healing had settled. Perfect nipple symmetry is reliable with this tattoo technique.
Keyhole Surgery
The Keyhole technique removes the fat and glandular chest tissue through a small incision under the nipple areola (minimally invasive). The main advantage of the keyhole technique is that you avoid the long horizontal scars on the chest. Other advantageous are: nipple sensation may be partially retained, and you avoid any issues with nipple grafts. Once the glandular tissue has been removed, the skin will stretch inwardly gradually after surgery, and follow the contour of the chest. Because the keyhole procedure doesn’t remove any skin, the risks are slightly higher of having fluid or blood build up underneath the skin in the ‘empty cavity’ created from surgery, when compared to double-incision technique (which removes skin and tightens the skin down more immediately by removing some skin). We can still avoid using drains for the keyhole procedure by using specialized internal dissolvable suture techniques.
The keyhole technique can only be offered to patients with a very small amount of chest tissue to be removed. They must also have very good skin elasticity that will stretch inwardly after the chest tissue is removed; otherwise, the chest skin will look like a wavy baggy sac of skin. Dr. Mckee is experienced in assessing whether or not you would be a candidate for the keyhole procedure, and the physical examination during the consultation will help decide this.
With the keyhole technique, major adjustments to the nipple size and shape cannot be performed at the same time as the surgery (because we need to maintain the nipple blood supply). Therefore, if any nipple adjustments are necessary/desired (such as nipple flattening, reducing diameter, re-positioning), we perform them safely as a second minor operation at a later date (3-12 months after the main keyhole procedure), and usually with the patient awake using only local anesthesia. With the double incision technique, there is greater precision in nipple size, nipple projection, and nipple position at the time of surgery – when compared to the keyhole technique.
Because the keyhole procedure is performed through a small incision (hole), visibility is slightly reduced compared to the double incision technique. Because of this limitation, there are slightly higher rates of general complications such as hematoma, seroma, infection, nipple position issues, small imperfections in chest skin contour/smoothness (little concavities, lumps, thinning, wrinkles, scars). There is also a higher need for a second procedure after the keyhole surgery, in order to adjust the nipple separately (higher need for revision surgery). The procedure takes slightly more time than double incision technique.
Which technique would be best for my specific body type?
Double Incision:
Double Incision technique can work with any body type.

This patient is a candidate for Double Incision, but not Keyhole surgery, based on the amount of chest tissue they have.
Keyhole:
You are only eligible for keyhole technique if you have a very small amount of chest tissue, AND you have skin elasticity that will recoil inwardly after the months following surgery. Also, if significant nipple modifications are desired at the time of surgery, the Double incision technique would be recommended instead of Keyhole.

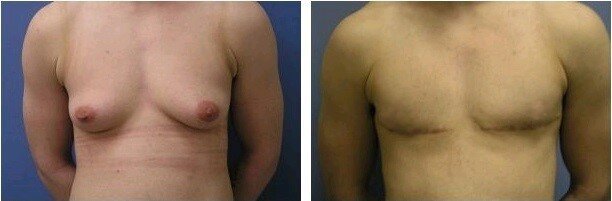
This patient is a candidate for either keyhole procedure, or Double Incision. They can choose which.
